Free Sfn 508 PDF Template
The SFN 508 form is a crucial document for individuals involved in early childhood services in North Dakota, specifically designed to ensure the safety and well-being of children. This form serves as an authorization for a background check related to child abuse and neglect, which is a vital step for anyone seeking employment in this sensitive field. It requires personal identifying information, including full legal name, address, and date of birth, to facilitate the background check process. Additionally, the form includes a certification section where applicants must affirm that they have not been convicted of crimes against children or felonies. This is not just a procedural step; it reflects the commitment to maintaining a safe environment for children. The form also grants permission for the North Dakota Department of Human Services to access relevant records from other states, ensuring a comprehensive review of an applicant's history. By consenting to the release of this information, individuals help safeguard the integrity of early childhood programs. Furthermore, the SFN 508 form addresses the need for transparency, requiring a signature to certify the accuracy of the provided information. Understanding the significance of this form is essential for anyone entering the early childhood services sector, as it underscores the importance of child safety and the responsibilities that come with working in this field.
Common PDF Documents
Neuroscience Meeting Planner 2023 - An accurate form contributes to smooth coordination between funeral services and legal requirements.
For those needing a comprehensive understanding of the process, the ADP Pay Stub document is indispensable, outlining critical information about earnings and deductions made during a designated pay period, while ensuring clarity and compliance in employee remuneration records.
Does a Small Estate Affidavit Need to Be Filed With the Court in California - Indicating whether the corporation is designed for perpetual existence or has a specified dissolution date is also necessary.
Similar forms
- SFN 509 - Child Care Provider Application: Similar to the SFN 508, this form collects personal information and background details to ensure that individuals working with children meet safety standards.
- California Bill of Sale Form: This form is essential for documenting the transfer of ownership of items in California, capturing crucial details such as item description, sale amount, and parties involved, ensuring legal validity of the transaction. For more information, you can access All California Forms.
- SFN 600 - Child Abuse and Neglect Reporting Form: This document is used to report suspected child abuse or neglect, requiring identifying information and details of the incident, similar to the SFN 508's focus on individual identification.
- SFN 622 - Criminal Background Check Authorization: Like the SFN 508, this form authorizes agencies to conduct background checks, ensuring that individuals have not committed crimes that would disqualify them from working with children.
- SFN 601 - Child Care Licensing Application: This application requires similar personal and employment history information to assess eligibility for child care licensing, paralleling the SFN 508’s purpose of ensuring safety in child care settings.
- SFN 512 - Child Care Provider Self-Declaration: This form allows individuals to declare their qualifications and background, much like the SFN 508, which requires self-certification of criminal history.
- SFN 507 - Background Check Consent Form: This document also seeks consent for background checks, emphasizing the importance of safety and compliance in early childhood services, similar to the SFN 508’s authorization sections.
How to Use Sfn 508
Completing the SFN 508 form is an important step in the process of obtaining a background check for child abuse and neglect. Follow these steps carefully to ensure that the form is filled out correctly.
- Begin by entering your full legal name in the designated field.
- Provide your address, including street and apartment number.
- If your mailing address differs from your residential address, fill in the mailing address section.
- Indicate the facility full legal name where you are applying.
- Enter your date of hire.
- Specify if you are a household member or a staff member.
- Fill in your city and state of residence, along with your ZIP code.
- Provide your email address.
- Enter your date of birth.
- List your home telephone number.
In the assurance section, certify that you have not been found guilty of a crime against children or convicted of a felony. If applicable, state your obligation to notify your employer or county social service board if such a situation arises.
- In the authorization for release of information section, grant permission for the North Dakota Department of Human Services and the County Social Service office to check your name in child abuse or neglect files.
- Consent to share any information found with Early Childhood Services staff and the director of the early childhood program.
- Authorize the release of information from other states where you have lived in the past ten years.
- List your Social Security number.
Next, provide any former addresses and the counties of residence where you have lived in the past ten years. Include any other names you have gone by in that same period.
- In the previous employment section, list any early childhood programs you have worked at in the last six months, including the county and dates employed.
Finally, certify the accuracy of the information by signing and dating the form. Remember to provide a copy of the completed form to the appropriate agencies as required.
Dos and Don'ts
When filling out the SFN 508 form for child abuse and neglect background checks, it’s essential to approach the process with care. Here’s a helpful list of things you should and shouldn’t do to ensure your application is completed correctly.
- Do provide accurate and complete identifying information, including your full legal name and address.
- Do read each section carefully before signing to ensure you understand your rights and responsibilities.
- Do notify your employer or county social service board immediately if you are found guilty of a crime against children.
- Do consent to the release of your information, as this is necessary for the background check process.
- Don't leave any fields blank, as incomplete forms may lead to delays or denials.
- Don't provide false information, as this could result in serious legal consequences.
- Don't forget to include your social security number, as it is mandatory for early childhood services operators.
- Don't ignore the importance of timely notification if your circumstances change after submitting the form.
By following these guidelines, you can help ensure that your application is processed smoothly and efficiently. Always remember that accuracy and honesty are paramount in these situations.
Document Example
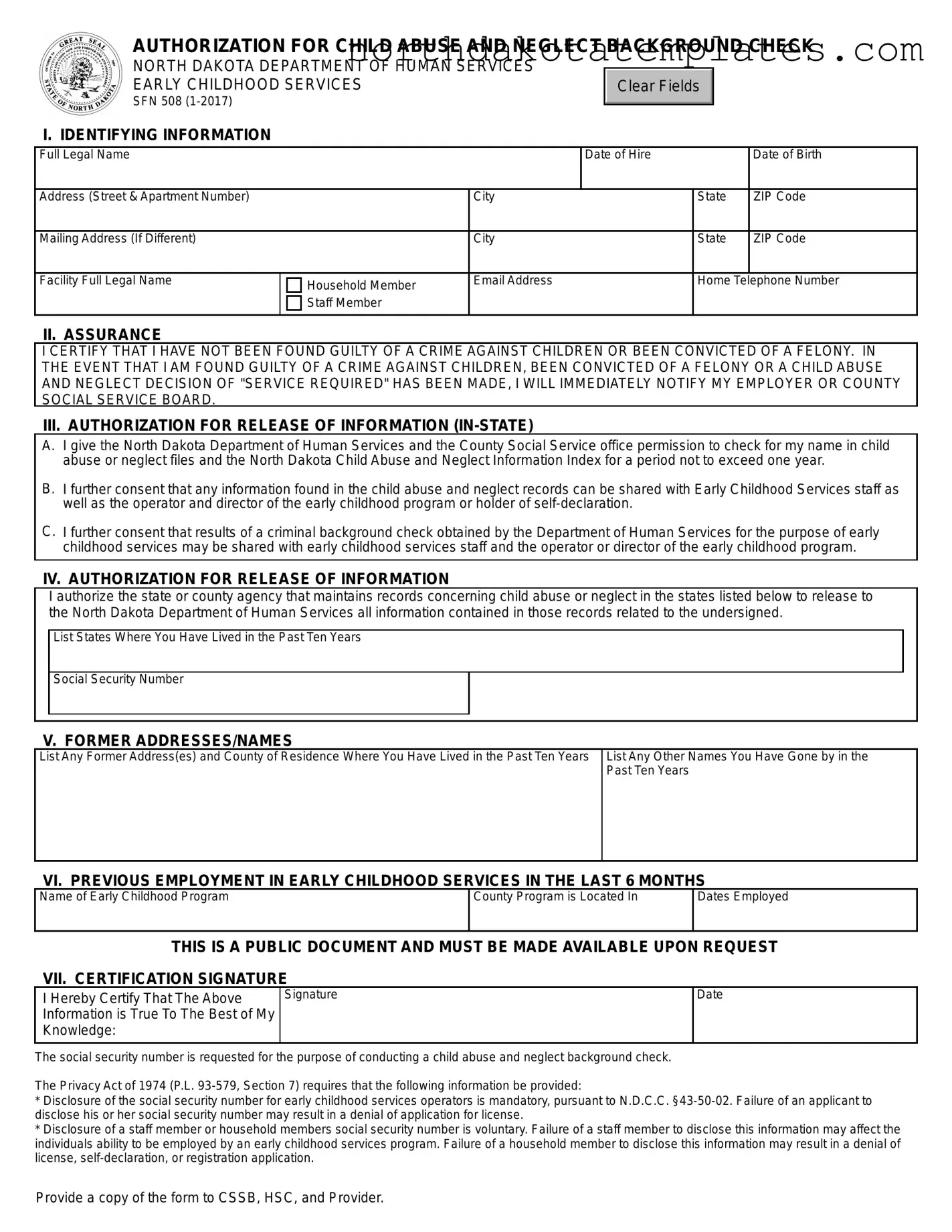
AUTHORIZATION FOR CHILD ABUSE AND NEGLECT BACKGROUND CHECK
NORTH DAKOTA DEPARTMENT OF HUMAN SERVICES EARLY CHILDHOOD SERVICES
SFN 508
Clear Fields
I. IDENTIFYING INFORMATION
Full Legal Name |
|
|
Date of Hire |
|
Date of Birth |
|
|
|
|
|
|
Address (Street & Apartment Number) |
|
City |
|
State |
ZIP Code |
|
|
|
|
|
|
Mailing Address (If Different) |
|
City |
State |
ZIP Code |
|
|
|
|
|
|
|
Facility Full Legal Name |
Household Member |
Email Address |
Home Telephone Number |
||
|
|
|
|
|
|
|
Staff Member |
|
|
|
|
|
|
|
|
|
|
II. ASSURANCE
I CERTIFY THAT I HAVE NOT BEEN FOUND GUILTY OF A CRIME AGAINST CHILDREN OR BEEN CONVICTED OF A FELONY. IN THE EVENT THAT I AM FOUND GUILTY OF A CRIME AGAINST CHILDREN, BEEN CONVICTED OF A FELONY OR A CHILD ABUSE AND NEGLECT DECISION OF "SERVICE REQUIRED" HAS BEEN MADE, I WILL IMMEDIATELY NOTIFY MY EMPLOYER OR COUNTY SOCIAL SERVICE BOARD.
III.AUTHORIZATION FOR RELEASE OF INFORMATION
A.I give the North Dakota Department of Human Services and the County Social Service office permission to check for my name in child abuse or neglect files and the North Dakota Child Abuse and Neglect Information Index for a period not to exceed one year.
B.I further consent that any information found in the child abuse and neglect records can be shared with Early Childhood Services staff as well as the operator and director of the early childhood program or holder of
C.I further consent that results of a criminal background check obtained by the Department of Human Services for the purpose of early childhood services may be shared with early childhood services staff and the operator or director of the early childhood program.
IV. AUTHORIZATION FOR RELEASE OF INFORMATION
I authorize the state or county agency that maintains records concerning child abuse or neglect in the states listed below to release to the North Dakota Department of Human Services all information contained in those records related to the undersigned.
List States Where You Have Lived in the Past Ten Years
Social Security Number
V. FORMER ADDRESSES/NAMES
List Any Former Address(es) and County of Residence Where You Have Lived in the Past Ten Years
List Any Other Names You Have Gone by in the Past Ten Years
VI. PREVIOUS EMPLOYMENT IN EARLY CHILDHOOD SERVICES IN THE LAST 6 MONTHS
Name of Early Childhood Program
County Program is Located In
Dates Employed
THIS IS A PUBLIC DOCUMENT AND MUST BE MADE AVAILABLE UPON REQUEST
VII. CERTIFICATION SIGNATURE
I Hereby Certify That The Above Information is True To The Best of My Knowledge:
Signature
Date
The social security number is requested for the purpose of conducting a child abuse and neglect background check.
The Privacy Act of 1974 (P.L.
*Disclosure of the social security number for early childhood services operators is mandatory, pursuant to N.D.C.C.
*Disclosure of a staff member or household members social security number is voluntary. Failure of a staff member to disclose this information may affect the individuals ability to be employed by an early childhood services program. Failure of a household member to disclose this information may result in a denial of license,
Provide a copy of the form to CSSB, HSC, and Provider.
SFN 508
Fingerprint Appointment Date
Fingerprints Completed Date
Results Memo Date
FOR OFFICAL USE ONLY
Regional Office
Child Abuse/Neglect Index Check
Date
Sexual Offender List
Date
Criminal Index
North Dakota Date
Minnesota Date
File Breakdown
| Fact Name | Details |
|---|---|
| Purpose | The SFN 508 form is used to authorize a background check for child abuse and neglect, ensuring the safety of children in early childhood services in North Dakota. |
| Governing Law | This form operates under North Dakota Century Code (N.D.C.C.) §43-50-02, which mandates the disclosure of social security numbers for early childhood services operators. |
| Information Required | Applicants must provide personal details such as full legal name, address, date of birth, and social security number, along with any prior addresses and names used in the last ten years. |
| Consent for Information Release | By signing the form, individuals consent to the release of their background check results and any relevant child abuse or neglect records to the North Dakota Department of Human Services and associated early childhood services staff. |
Common mistakes
When individuals fill out the SFN 508 form for child abuse and neglect background checks, several common mistakes can hinder the process. One significant error is providing incomplete identifying information. The form requires full legal names, addresses, and contact details. Omitting any of these details can lead to delays in processing or even rejection of the application. Ensuring all fields are filled accurately is crucial for a smooth review.
Another frequent mistake involves the failure to list all former addresses and names. The form specifically asks for a history of addresses and any other names used in the past ten years. Neglecting to provide this information can raise red flags during the background check. It is essential to be thorough and transparent, as discrepancies may lead to further scrutiny.
Individuals often overlook the importance of the certification section. This section requires a signature and date, affirming that the information provided is true to the best of the individual's knowledge. Failing to sign or date the form can result in the application being considered incomplete. This simple oversight can cause significant delays in the background check process.
Lastly, some applicants misunderstand the requirements regarding the social security number. While the disclosure of this number is mandatory for early childhood services operators, it is voluntary for staff members and household members. Misunderstanding this distinction can lead to unnecessary complications. Applicants should be aware of the implications of providing or withholding this information, as it can affect employment opportunities and licensing outcomes.
FAQ
What is the purpose of the SFN 508 form?
The SFN 508 form is used to authorize a background check for child abuse and neglect. This form is essential for individuals seeking employment in early childhood services in North Dakota. By completing this form, applicants allow the North Dakota Department of Human Services and local social service offices to check their names against child abuse and neglect records. This process helps ensure the safety and well-being of children in early childhood programs.
Who needs to fill out the SFN 508 form?
Anyone applying for a position in early childhood services in North Dakota must complete the SFN 508 form. This includes staff members and household members who may have access to children in these programs. The form is designed to gather identifying information, employment history, and consent for background checks. It is crucial for maintaining a safe environment for children.
What information is required on the SFN 508 form?
The SFN 508 form requires various pieces of information. Applicants must provide their full legal name, address, date of birth, and contact information. Additionally, they need to list any former addresses and names used in the past ten years. The form also asks for details about previous employment in early childhood services, if applicable. Importantly, it includes a section for the applicant to certify that they have not been found guilty of any crimes against children or convicted of felonies.
What happens if someone does not provide their social security number on the SFN 508 form?
Providing a social security number is mandatory for early childhood services operators, as specified by North Dakota law. If an applicant fails to disclose their social security number, it may lead to a denial of their application for a license. For staff members and household members, disclosure is voluntary. However, not providing this information could affect their ability to be employed in an early childhood services program. It is essential to understand the implications of not providing this information when filling out the form.