Free Sfn 50645 PDF Template
The SFN 50645 form, officially known as the Certified Nurse Aide Registry Endorsement, is a crucial document for individuals seeking to maintain or transfer their certification as a nurse aide in North Dakota. This form is managed by the North Dakota Department of Health, specifically within the Division of Health Facilities, and serves multiple important purposes. Primarily, it allows certified nurse aides to report their employment history across various states, ensuring that their credentials are recognized and endorsed appropriately. The form requires personal information, including the applicant's Social Security number, contact details, and date of birth. It also prompts applicants to disclose any past criminal history, disciplinary actions, or health issues that could impact their ability to perform their duties safely and effectively. Each question on the form is designed to gather comprehensive information about the applicant's background and professional conduct, which is vital for maintaining the integrity of the nurse aide registry. Completing the SFN 50645 form accurately and thoroughly is essential for those looking to continue their careers in the healthcare field, as it plays a significant role in the endorsement process and ultimately impacts patient care standards in North Dakota.
Common PDF Documents
Sfn 12011 - Make sure to disclose any past license denials or suspensions in the application.
Filing the Florida Articles of Incorporation form is essential for anyone looking to establish a corporation within the state, as it provides the foundational information necessary for registration with the Florida Department of State. This document includes critical details such as the corporation’s name, address, and directors, making it the first official step in creating a recognized business entity in Florida. For more information, you can refer to the detailed guide at https://floridaforms.net/blank-articles-of-incorporation-form.
Neuroscience Meeting Planner 2023 - The form assures compliance with North Dakota state regulations on disposition.
Similar forms
- Nurse Aide Registry Application: Similar to the SFN 50645 form, this application is essential for individuals seeking to become certified nurse aides. It collects personal information, work history, and any disciplinary actions, ensuring that applicants meet the necessary qualifications for certification.
- Background Check Authorization Form: This document serves to authorize a background check on the applicant. Like the SFN 50645, it addresses any criminal history, which is crucial for ensuring the safety of patients and compliance with state regulations.
- Continuing Education Verification Form: This form is used to verify that certified nurse aides have completed the required continuing education. It parallels the SFN 50645 in that it confirms ongoing competency and compliance with state requirements for maintaining certification.
- Renewal Application for Nursing License: Much like the SFN 50645, this application requires personal details and information regarding any disciplinary actions or legal issues that may affect licensure. Both forms are necessary for maintaining professional standing in the healthcare field.
- Employment Verification Form: This document is often required by regulatory bodies to confirm an individual's employment history in healthcare. It shares similarities with the SFN 50645 in that it emphasizes the importance of accurate and truthful reporting of work experience.
- California Last Will and Testament Form: This legal document allows individuals to dictate the distribution of their assets after death, ensuring wishes are respected and minimizing family disputes. For more details, you can visit All California Forms.
- Health Assessment Form: This form collects information about the applicant's physical and mental health, similar to the health-related questions found in the SFN 50645. Both documents are designed to ensure that individuals are fit to provide care without risking patient safety.
How to Use Sfn 50645
Filling out the SFN 50645 form is an important step in the process of seeking endorsement for the Certified Nurse Aide Registry in North Dakota. Ensure all required information is accurate and complete before submission.
- Begin by entering your Social Security Number at the top of the form.
- List the states where you are certified in the designated fields.
- Provide the Last Date Worked and indicate the respective state for each job.
- Fill in your Nurse Aide Registry Number if applicable.
- Enter your First Name, Last Name, and Maiden/Middle Name (if any).
- Indicate your Gender by marking M for Male or F for Female.
- Provide your Date of Birth.
- Fill in your Current Mailing Address, including City, State, Zip, and County.
- Enter your Daytime Phone number and E-Mail Address.
- If applicable, include your ND CNA #.
- Complete the section regarding the Nurse Aide Program Completed, including the facility name, city, and date completed.
- Record Today’s Date.
- Answer all questions regarding any arrests, charges, or convictions truthfully.
- If you answer “Yes” to any questions, attach a detailed written explanation and any relevant legal documents.
- Confirm that you have attached the appropriate documents, if required.
- Choose your submission method: E-mail to naregistry@nd.gov, FAX to 701.328.1890, or MAIL to CNA Registry, 600 E. Boulevard Ave., Dept. 301, Bismarck, N.D., 58505-0200.
Dos and Don'ts
When filling out the SFN 50645 form, keep the following tips in mind:
- Do read the entire form carefully before starting.
- Do provide accurate and complete information for each section.
- Do answer all questions honestly, especially regarding your background.
- Do attach any required documents if you answered "Yes" to specific questions.
- Do double-check your contact information for accuracy.
- Don't leave any questions unanswered; all fields must be completed.
- Don't provide false information; this can lead to denial of your application.
- Don't forget to sign and date the form before submission.
- Don't submit the form without reviewing it for errors.
- Don't ignore the submission methods; follow the instructions for emailing, faxing, or mailing.
Document Example
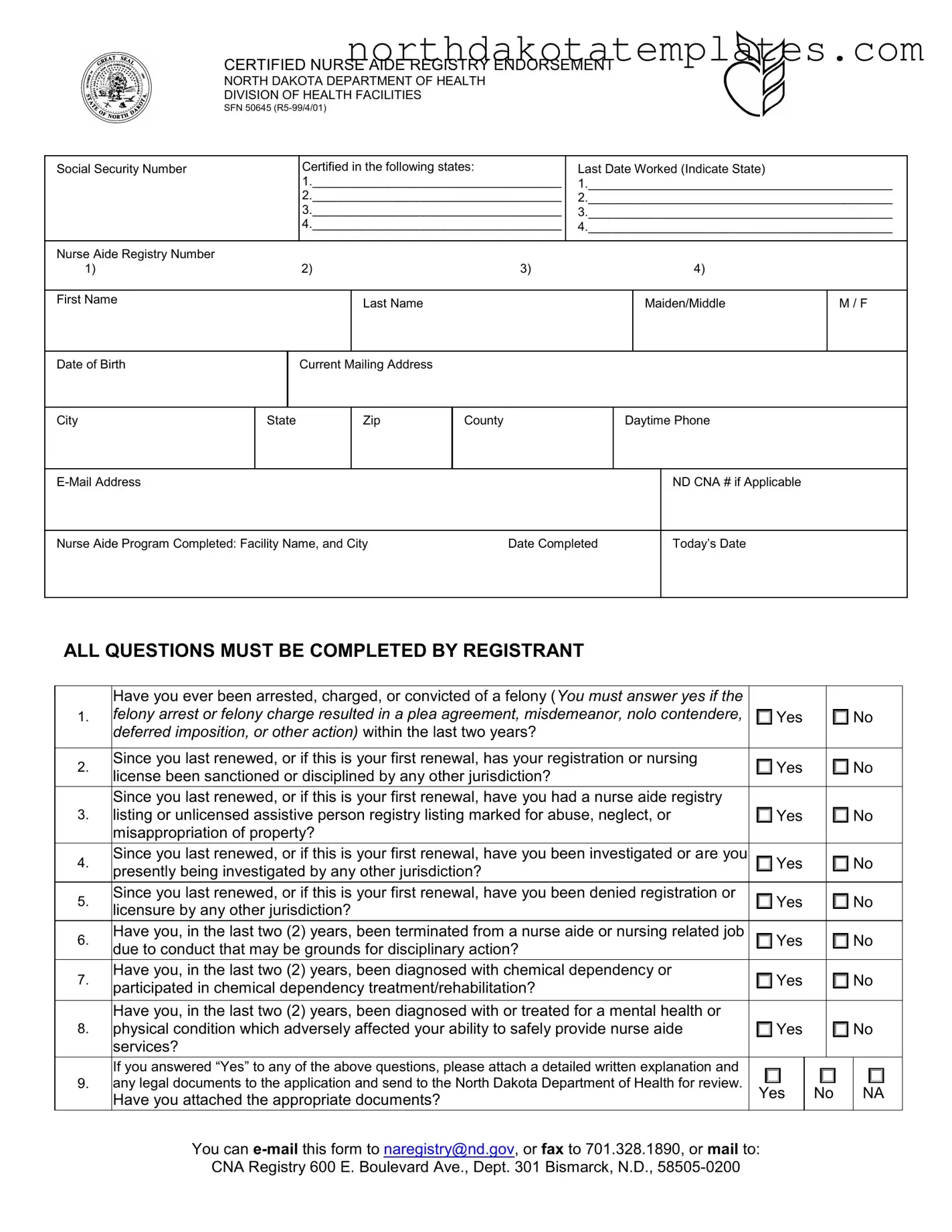
CERTIFIED NURSE AIDE REGISTRY ENDORSEMENT
NORTH DAKOTA DEPARTMENT OF HEALTH
DIVISION OF HEALTH FACILITIES
SFN 50645
Social Security Number |
|
|
Certified in the following states: |
Last Date Worked (Indicate State) |
|
|||||
|
|
|
1.____________________________________ |
1.____________________________________________ |
||||||
|
|
|
2.____________________________________ |
2.____________________________________________ |
||||||
|
|
|
3.____________________________________ |
3.____________________________________________ |
||||||
|
|
|
4.____________________________________ |
4.____________________________________________ |
||||||
|
|
|
|
|
|
|
|
|
|
|
Nurse Aide Registry Number |
|
|
|
|
|
|
|
|
|
|
1) |
|
|
2) |
|
3) |
|
4) |
|
||
|
|
|
|
|
|
|
|
|
|
|
First Name |
|
|
|
Last Name |
|
|
|
Maiden/Middle |
M / F |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
Date of Birth |
|
|
Current Mailing Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
State |
|
Zip |
County |
|
Daytime Phone |
|
|||
ALL QUESTIONS MUST |
BE REG |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ND CNA # if Applicable |
|
|
|
|
|
|
|
|
|
||||
Nurse Aide Program Completed: Facility Name, and City |
Date Completed |
|
|
Today’s Date |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
ALL QUESTIONS MUST BE COMPLETED BY REGISTRANT
Have you ever been arrested, charged, or convicted of a felony (You must answer yes if the
1.felony arrest or felony charge resulted in a plea agreement, misdemeanor, nolo contendere, Yes No deferred imposition, or other action) within the last two years?
2. |
Since you last renewed, or if this is your first renewal, has your registration or nursing |
|
Yes |
|
No |
|
license been sanctioned or disciplined by any other jurisdiction? |
|
|||||
|
|
|
|
|
|
|
|
Since you last renewed, or if this is your first renewal, have you had a nurse aide registry |
|
|
|
|
|
3. |
listing or unlicensed assistive person registry listing marked for abuse, neglect, or |
Yes |
|
No |
||
|
misappropriation of property? |
|
|
|
|
|
4. |
Since you last renewed, or if this is your first renewal, have you been investigated or are you |
|
Yes |
|
|
No |
|
presently being investigated by any other jurisdiction? |
|
|
|
|
|
5. |
Since you last renewed, or if this is your first renewal, have you been denied registration or |
|
Yes |
|
|
No |
|
licensure by any other jurisdiction? |
|
|
|
|
|
6. |
Have you, in the last two (2) years, been terminated from a nurse aide or nursing related job |
|
Yes |
|
No |
|
|
due to conduct that may be grounds for disciplinary action? |
|
|
|
|
|
7. |
Have you, in the last two (2) years, been diagnosed with chemical dependency or |
|
Yes |
|
|
No |
participated in chemical dependency treatment/rehabilitation? |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Have you, in the last two (2) years, been diagnosed with or treated for a mental health or |
|
|
|
|
|
8. |
physical condition which adversely affected your ability to safely provide nurse aide |
Yes |
|
No |
||
|
services? |
|
|
|
|
|
|
If you answered “Yes” to any of the above questions, please attach a detailed written explanation and |
|
|
|
|
|
9. |
any legal documents to the application and send to the North Dakota Department of Health for review. |
|
||||
Yes |
No |
NA |
||||
|
Have you attached the appropriate documents? |
|
|
|
|
|
|
You can |
|
|
|
|
|
|
CNA Registry 600 E. Boulevard Ave., Dept. 301 Bismarck, N.D., |
|
|
|
|
|
File Breakdown
| Fact Name | Description |
|---|---|
| Purpose | The SFN 50645 form is used for Certified Nurse Aide Registry endorsement in North Dakota. |
| Governing Law | This form is governed by North Dakota Century Code, Chapter 43-12.1. |
| Eligibility | Applicants must provide their Social Security Number and details about their nurse aide training. |
| Background Questions | The form includes questions regarding criminal history and professional conduct over the past two years. |
| Submission Methods | Applicants can submit the form via email, fax, or mail to the North Dakota Department of Health. |
| Contact Information | For inquiries, the email address is naregistry@nd.gov and the fax number is 701.328.1890. |
Common mistakes
Filling out the SFN 50645 form can be a straightforward process, but many people stumble due to common mistakes. One significant error occurs when individuals fail to provide complete information. Every section of the form must be filled out accurately. Omitting details, such as the last date worked or the facility name, can lead to delays in processing or even rejection of the application.
Another frequent mistake is misunderstanding the questions regarding criminal history. Some applicants may answer "No" to questions about arrests or convictions without realizing that even a plea agreement or deferred imposition counts as a felony charge. It's crucial to read these questions carefully and answer truthfully. Failing to disclose relevant information can have serious consequences, including potential legal ramifications.
People often neglect to include the necessary documentation when submitting their application. If you answer "Yes" to any of the questions about past conduct or issues, you must attach a detailed explanation and any relevant legal documents. Forgetting to do this can result in an incomplete application, which will not be processed until all required information is provided.
Another common oversight is incorrect personal information. Ensure that your name, Social Security number, and contact details are accurate. Errors in this information can lead to complications in communication and delays in the application process. Double-checking these details can save time and frustration.
Additionally, some applicants may not be aware of the importance of including their Nurse Aide Registry Number if applicable. This number is essential for verifying your credentials and ensuring that your application is processed correctly. Missing this information can slow down the review process.
Lastly, failing to follow submission guidelines can hinder the application process. Whether you choose to email, fax, or mail your form, make sure you adhere to the specified instructions. Each method has its own requirements, and not following them can result in your application being lost or delayed. Taking the time to review the submission process thoroughly can prevent unnecessary complications.
FAQ
What is the purpose of the SFN 50645 form?
The SFN 50645 form is used for the Certified Nurse Aide Registry Endorsement in North Dakota. This form allows individuals who are certified nurse aides in other states to apply for registration in North Dakota. It ensures that the applicant meets the necessary requirements and standards for providing care in the state. By completing this form, you help maintain the quality of care provided to patients and ensure that all nurse aides are properly vetted before they begin working in healthcare facilities.
What information do I need to provide on the form?
You will need to provide personal information, including your name, date of birth, and contact details. Additionally, you must list your previous certifications and the states where you have worked as a nurse aide. The form also requires you to answer questions regarding your criminal history, any disciplinary actions taken against your nursing license, and any health-related issues that may affect your ability to perform nurse aide duties. It is essential to answer these questions honestly, as they are crucial for your application review.
How do I submit the SFN 50645 form?
You have several options for submitting the SFN 50645 form. You can email it to naregistry@nd.gov, fax it to 701.328.1890, or mail it to the North Dakota Department of Health at the address provided on the form. Make sure to attach any necessary documents, especially if you answered "Yes" to any of the questions regarding your background or health. Submitting all required information accurately will help expedite the processing of your application.
What happens after I submit the form?
Once you submit the SFN 50645 form, it will be reviewed by the North Dakota Department of Health. They will evaluate your application based on the information provided and any attached documents. If any issues arise during the review, you may be contacted for further clarification or additional information. If your application is approved, you will receive your nurse aide registry number, allowing you to work as a certified nurse aide in North Dakota. It is important to keep an eye on your email or mail for any updates regarding your application status.