Free North Dakota Ems Patient Care Report PDF Template
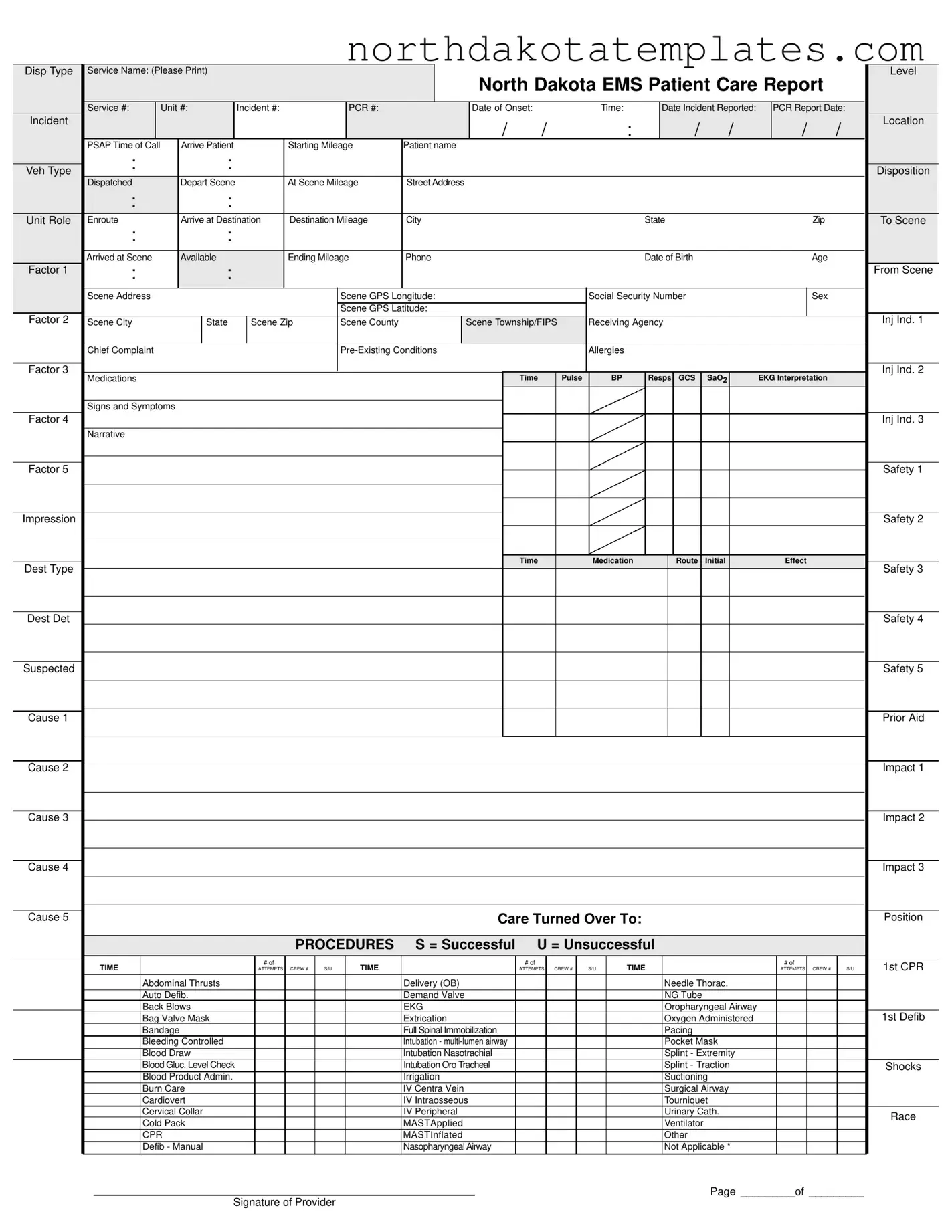
The North Dakota EMS Patient Care Report form is a crucial document that captures essential information during emergency medical services. This form includes various fields that help paramedics and medical personnel document patient care and incident details accurately. Key sections cover service identification, incident specifics, and patient demographics, ensuring that all relevant data is collected. Important metrics such as vital signs, medications administered, and procedures performed are also recorded. Additionally, the form addresses billing information, allowing for efficient processing of insurance claims. It includes sections for documenting the patient's chief complaint, pre-existing conditions, and allergies, which are vital for effective treatment. The report also emphasizes safety protocols and the transfer of care to receiving agencies. By organizing this information systematically, the form facilitates communication among healthcare providers and ensures a comprehensive approach to patient care.
Common PDF Documents
How Do I Get My 1099-g Online California - Granting the percent of acquired assets or workforce from previously owned businesses must be clearly outlined in the submission.
In addition to the Bill of Sale form, it's important to familiarize yourself with various relevant documents to streamline your transactions. For comprehensive resources, you can check All Arizona Forms to ensure you have everything necessary for a smooth and legal sale process.
Society for Neuroscience - Completing the SFN 509 form is an important step for out-of-state facilities aiming to access Medicaid funding.
Similar forms
- Emergency Medical Services (EMS) Run Report: Similar to the North Dakota EMS Patient Care Report, this document details the services provided during an emergency response, including patient information, treatment administered, and outcomes.
- Patient Care Record (PCR): This form captures similar patient data, including demographics, medical history, and treatment details, ensuring continuity of care across medical providers.
- Ambulance Trip Report: This report outlines the specifics of the ambulance trip, including times of dispatch, arrival, and departure, mirroring the timeline elements found in the EMS Patient Care Report.
- Pre-Hospital Care Report: Like the North Dakota form, this document records the pre-hospital care provided to the patient, detailing assessments and interventions performed by EMS personnel.
- Hospital Admission Form: This form collects similar information upon patient admission, including medical history and treatment details, facilitating a smooth transition from EMS to hospital care.
Bill of Sale Form: To facilitate legal asset transactions, refer to our comprehensive bill of sale form guide for thorough documentation.
- Incident Report: This document provides a comprehensive account of the incident, including circumstances and actions taken, paralleling the narrative section of the EMS Patient Care Report.
- Insurance Claim Form: This form requires similar patient and treatment information for billing purposes, ensuring that the necessary details for reimbursement are documented.
How to Use North Dakota Ems Patient Care Report
Completing the North Dakota EMS Patient Care Report form is crucial for documenting patient care and ensuring accurate billing. Follow these steps to fill out the form correctly.
- Start by printing your Service Name and Service # at the top of the form.
- Fill in the Unit #, Incident #, and PCR #.
- Record the Date of Onset and Time of the incident.
- Document the Date Incident Reported and PCR Report Date.
- Provide the Location and PSAP Time of Call.
- Fill in Arrive, Depart Scene, and At Scene Mileage.
- Enter the Patient name, Date of Birth, Age, and Sex.
- Document the Scene Address, City, State, Zip, and County.
- Record Social Security Number and Scene GPS Longitude and Latitude.
- Fill in the Chief Complaint, Pre-Existing Conditions, and Allergies.
- Document medications, vital signs, and any signs and symptoms.
- Complete the Narrative section with details about the patient’s condition.
- Fill in the Procedures section, noting the success or failure of each attempt.
- Document Billing Information including insurance type and responsible party details.
- Complete the Receipt of Service or Refusal of Service section as applicable.
- Finally, ensure all crew member names and their roles are recorded.
After completing the form, review it for accuracy. Ensure all required fields are filled and signatures are obtained where necessary. This will help facilitate a smooth process for both patient care and billing.
Dos and Don'ts
When filling out the North Dakota EMS Patient Care Report form, it is crucial to ensure accuracy and completeness. Here’s a list of things to do and avoid:
- Do print clearly to ensure all information is legible.
- Do double-check all entries for accuracy before submission.
- Do include all relevant patient details, such as name, date of birth, and address.
- Do document the time and date of the incident and when the report is filed.
- Do specify the chief complaint and any pre-existing conditions the patient may have.
- Don't leave any sections blank unless instructed otherwise.
- Don't use abbreviations that may not be universally understood.
- Don't forget to sign the report, as this validates the information provided.
- Don't submit the form without ensuring that all required signatures are obtained.
Document Example
Disp Type |
Service Name: (Please Print) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Level |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
North Dakota EMS Patient Care Report |
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Service #: |
|
Unit #: |
Incident #: |
|
|
|
PCR #: |
|
|
|
Date of Onset: |
|
|
Time: |
|
|
Date Incident Reported: |
|
PCR Report Date: |
|
||||||||||||||||||
Incident |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
: |
|
/ |
|
/ |
|
/ |
|
/ |
Location |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
PSAP Time of Call |
|
Arrive Patient |
|
|
|
Starting Mileage |
Patient name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
: |
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Veh Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Disposition |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Dispatched |
|
Depart Scene |
|
|
|
At Scene Mileage |
Street Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
: |
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unit Role |
Enroute |
|
Arrive at Destination |
Destination Mileage |
City |
|
|
|
|
|
|
|
State |
|
|
|
|
|
Zip |
|
|
To Scene |
|||||||||||||||||
|
: |
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Arrived at Scene |
|
Available |
|
|
|
Ending Mileage |
Phone |
|
|
|
|
|
|
|
Date of Birth |
|
|
|
|
|
Age |
|
|
|
||||||||||||||
Factor 1 |
: |
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
From Scene |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Scene Address |
|
|
|
|
|
|
|
|
Scene GPS Longitude: |
|
|
|
|
Social Security Number |
|
|
|
|
|
Sex |
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Scene GPS Latitude: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Factor 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Inj Ind. 1 |
Scene City |
|
|
State |
|
Scene Zip |
|
Scene County |
|
|
Scene Township/FIPS |
Receiving Agency |
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chief Complaint |
|
|
|
|
|
|
|
|
|
|
|
|
Allergies |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Factor 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Inj Ind. 2 |
|
Medications |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Time |
Pulse |
|
BP |
|
Resps |
GCS |
|
SaO2 |
|
EKG Interpretation |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signs and Symptoms |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Factor 4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Inj Ind. 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Narrative |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Factor 5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Impression |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Time |
|
|
Medication |
|
|
|
Route |
|
Initial |
|
|
|
Effect |
|
|
|
||||
Dest Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 3 |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dest Det |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Suspected |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Prior Aid |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Impact 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Impact 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Impact 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Care Turned Over To: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Position |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PROCEDURES |
S = Successful |
U = Unsuccessful |
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
# of |
|
|
|
|
|
|
|
|
|
# of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
# of |
|
|
|
|
|
TIME |
|
|
|
|
|
|
|
|
|
|
TIME |
|
|
|
|
|
|
|
|
|
|
TIME |
|
|
|
|
|
|
|
|
|
|
1st CPR |
|||||
|
|
|
|
|
|
|
|
ATTEMPTS |
CREW # |
S/U |
|
|
|
|
|
|
ATTEMPTS |
|
CREW # |
|
S/U |
|
|
|
|
|
|
|
|
ATTEMPTS |
CREW # |
|
S/U |
||||||
|
|
Abdominal Thrusts |
|
|
|
|
|
|
|
Delivery (OB) |
|
|
|
|
|
|
|
|
|
Needle Thorac. |
|
|
|
|
|
|
|
||||||||||||
|
|
Auto Defib. |
|
|
|
|
|
|
|
Demand Valve |
|
|
|
|
|
|
|
|
|
NG Tube |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Back Blows |
|
|
|
|
|
|
|
EKG |
|
|
|
|
|
|
|
|
|
Oropharyngeal Airway |
|
|
|
|
|
|
|
||||||||||||
|
|
Bag Valve Mask |
|
|
|
|
|
|
|
Extrication |
|
|
|
|
|
|
|
|
|
Oxygen Administered |
|
|
|
|
|
|
1st Defib |
||||||||||||
|
|
Bandage |
|
|
|
|
|
|
|
Full Spinal Immobilization |
|
|
|
|
|
|
|
|
|
Pacing |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Bleeding Controlled |
|
|
|
|
|
|
|
Intubation - |
|
|
|
|
|
|
|
|
|
Pocket Mask |
|
|
|
|
|
|
|
||||||||||||
|
|
Blood Draw |
|
|
|
|
|
|
|
Intubation Nasotrachial |
|
|
|
|
|
|
|
|
|
Splint - Extremity |
|
|
|
|
|
|
|
||||||||||||
|
|
Blood Gluc. Level Check |
|
|
|
|
|
|
|
Intubation Oro Tracheal |
|
|
|
|
|
|
|
|
|
Splint - Traction |
|
|
|
|
|
|
Shocks |
||||||||||||
|
|
Blood Product Admin. |
|
|
|
|
|
|
|
Irrigation |
|
|
|
|
|
|
|
|
|
Suctioning |
|
|
|
|
|
|
|
||||||||||||
|
|
Burn Care |
|
|
|
|
|
|
|
IV Centra Vein |
|
|
|
|
|
|
|
|
|
Surgical Airway |
|
|
|
|
|
|
|
||||||||||||
|
|
Cardiovert |
|
|
|
|
|
|
|
IV Intraosseous |
|
|
|
|
|
|
|
|
|
Tourniquet |
|
|
|
|
|
|
|
||||||||||||
|
|
Cervical Collar |
|
|
|
|
|
|
|
IV Peripheral |
|
|
|
|
|
|
|
|
|
Urinary Cath. |
|
|
|
|
|
|
Race |
||||||||||||
|
|
Cold Pack |
|
|
|
|
|
|
|
MASTApplied |
|
|
|
|
|
|
|
|
|
Ventilator |
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
CPR |
|
|
|
|
|
|
|
MASTInflated |
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Defib - Manual |
|
|
|
|
|
|
|
Nasopharyngeal Airway |
|
|
|
|
|
|
|
|
|
Not Applicable * |
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page _________of _________
Signature of Provider
Patient Name (PLEASE PRINT)
North Dakota EMS Patient Care Report
|
|
|
BILLING INFORMATION |
|
|
|
|
|
|
MILEAGE |
|
INSURANCE TYPE |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insurance - Primary |
Number: |
Insurance - Secondary |
Number: |
|
Beg: |
|
|
|
❏ No Insurance |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ Private Pay |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Responsible Party: |
|
|
|
|
|
|
|
End: |
|
|
|
❏ Private Insurance |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ Medicare |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Last Name) |
|
(First Name) |
|
|
|
(MI) |
|
Total: |
|
|
|
❏ Medicaid |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ Medicare/Medicaid |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Address) |
|
|
|
|
|
|
|
|
|
|
|
❏ VA Insurance |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(City) |
(State) |
(Zip) |
|
|
(Phone) |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ Not Applicable |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RECEIPT OF SERVICE |
|
|
|
|
|
|
REFUSAL OF SERVICE |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
I acknowledge receipt of the EMS services listed in this document and accept |
This is to certify that I am refusing treatment / transport. I have been informed |
|||||||||||||
|
full responsibility for all charges. I authorize payment of medical benefits from |
of the risk(s) involved, and hereby release the ambulance service, its atten- |
|||||||||||||
|
my insurance company to provide of such services and authorize the provider |
dants, and its affiliates, from all responsibility which may result from this action. |
|||||||||||||
|
to release medical and other necessary information to my insurance company |
|
|
|
|
|
|
|
|
|
|||||
|
for that purpose. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Patient Signature |
|
|
Date/Time |
Patient Signature |
|
|
|
Date/Time |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CREW |
|
CREW MEMBER NAMES |
|
|
|
|
STAFF ID |
|
DRIVER |
LEVEL |
||||
1 |
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EKG STRIPS
File Breakdown
| Fact Name | Details |
|---|---|
| Service Identification | The North Dakota EMS Patient Care Report includes fields for service name, service number, and unit number to identify the responding EMS service. |
| Incident Information | Key details such as incident number, date of onset, and time of call are required to document the event accurately. |
| Patient Details | Information like patient name, date of birth, age, and social security number must be recorded to ensure proper care and billing. |
| Procedures and Treatments | The form outlines various procedures performed, including CPR, intubation, and medication administration, along with their success rates. |
| Governing Law | The North Dakota EMS Patient Care Report is governed by North Dakota Century Code § 23-27-01, which regulates emergency medical services. |
Common mistakes
Filling out the North Dakota EMS Patient Care Report form accurately is crucial for effective patient care and documentation. However, there are common mistakes that individuals often make during this process. Recognizing these pitfalls can help ensure that the report is completed correctly.
One frequent error is neglecting to provide complete patient information. Essential details such as the patient's name, date of birth, and social security number must be filled out accurately. Omitting this information can lead to difficulties in patient identification and billing issues later on.
Another common mistake involves inaccurate recording of the incident details. This includes the date and time of the incident, as well as the location. If these details are incorrect, it may complicate the response and follow-up care for the patient. Always double-check these entries for accuracy.
Many people also fail to document the chief complaint and pre-existing conditions properly. These elements are vital for understanding the patient's medical history and the context of the emergency. Incomplete information in this section can hinder the medical team's ability to provide appropriate care.
Additionally, errors often occur in the section detailing the medications administered. It is essential to record the correct medications, dosages, and routes of administration. Miscommunication in this area can lead to dangerous outcomes for the patient.
Another mistake is related to the procedures performed. Individuals may forget to indicate whether a procedure was successful or unsuccessful. This information is critical for future medical evaluations and can affect ongoing treatment plans.
Some people mistakenly leave out the billing information or do not provide complete insurance details. This can result in delays in payment and potential financial complications for the patient. It is important to ensure that all insurance information is accurately recorded.
Moreover, individuals often overlook the signature section. Both the patient and the provider must sign the report to validate the information and authorize treatment. Missing signatures can render the report incomplete and may lead to legal issues.
Lastly, failing to include detailed narratives of the incident and care provided is a common oversight. A thorough narrative helps to create a complete picture of the event and the actions taken, which is vital for both legal and medical reasons.
By being aware of these common mistakes, individuals can ensure that the North Dakota EMS Patient Care Report form is filled out correctly, leading to better patient care and documentation practices.
FAQ
What is the North Dakota EMS Patient Care Report form used for?
The North Dakota EMS Patient Care Report form serves as a comprehensive documentation tool for emergency medical services. It captures vital information about the patient, the incident, and the care provided. This report is essential for ensuring continuity of care, facilitating billing, and meeting legal and regulatory requirements. It helps EMS personnel communicate effectively with other healthcare providers and ensures that patient information is accurately recorded for future reference.
What information is required on the form?
The form requires various details, including the service name, unit number, incident number, and patient information such as name, date of birth, and social security number. Additionally, it collects information about the incident itself, including the time and location, chief complaint, pre-existing conditions, allergies, and medications. Documentation of the care provided, such as procedures performed and vital signs, is also crucial. This comprehensive data collection is vital for both patient care and billing purposes.
How does the billing information section work?
The billing information section of the form is designed to capture insurance details for the patient. It includes spaces for primary and secondary insurance numbers, as well as options for various types of coverage, such as private insurance, Medicare, and Medicaid. This section ensures that the EMS provider can bill the appropriate insurance company for the services rendered. Accurate completion of this section is important for timely reimbursement and to avoid billing errors.
What should I do if I refuse treatment or transport?
If a patient chooses to refuse treatment or transport, they must complete the designated section of the form that certifies their decision. This section requires the patient to acknowledge that they have been informed of the risks involved in refusing care. By signing this section, the patient releases the EMS service and its personnel from any responsibility that may arise from their decision. It is crucial for patients to understand the implications of their choice and to communicate their wishes clearly.
How is patient confidentiality maintained with this form?